Transforming Outpatient Care: Grampian's Digital Appointments Study
This project was funded by the Health Foundation
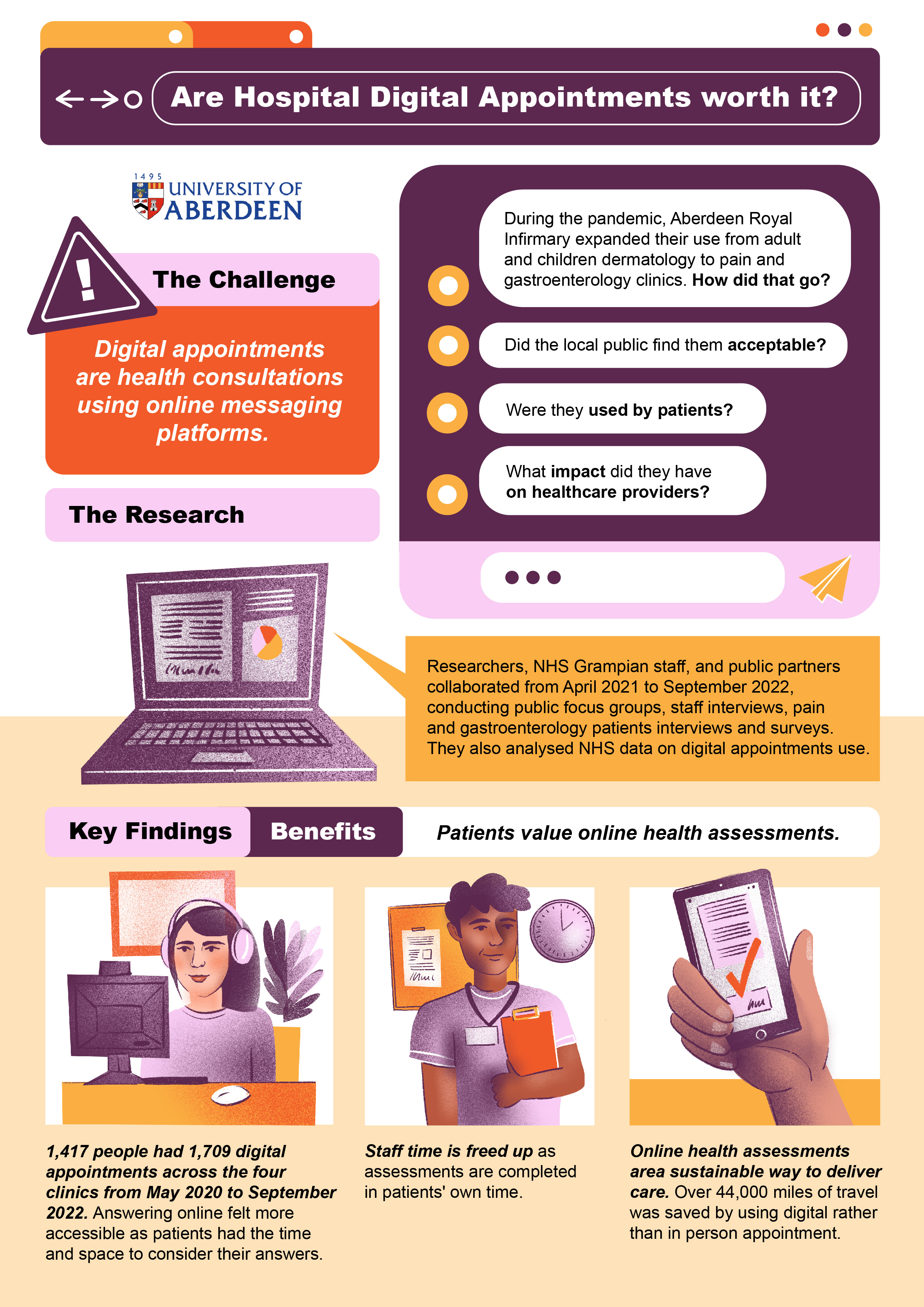
During the pandemic, healthcare underwent a significant transformation. Many traditional face-to-face appointments in outpatient care were replaced by video and phone consultations. Another option introduced was asynchronous consultations, where patients fill out an online form detailing important clinical information at their convenience, which is later reviewed by a health professional. A decision is then made about what the best next steps are which can include further investigations or discharge.
Starting in December 2021, the pain management service clinic at the Aberdeen Royal Infirmary adopted asynchronous consultations (known as ‘digital appointments’). Then, a couple of months after some Gastroenterology (stomach and gut) and Pain clinics started using it too. They were inspired by the Dermatology (skin health) outpatient service, which had been using this approach since May 2020. These changes to the way care was being delivered served as a unique opportunity to understand public readiness for this new NHS service as well as its impact on both staff and patients, to help determine its future use across the NHS.
A team of researchers from the University of Aberdeen, innovation leaders from NHS Grampian, and members of the public, came together to provide a rounded picture of this new service development and adoption as it happened. It is important because a service that is not accepted by the public, wanted by patients, or efficiently used by staff will likely fail or at least not have the most helpful impact possible.
What is the big deal with digital appointments?
Even before the pandemic, remote communication methods, including video calls and emails, were on the rise in healthcare settings, especially in Scotland. The pandemic fast-tracked this evolution, enabling patients who are not in need of urgent care to receive care remotely. Asynchronous consultations emerged as one of the alternatives to traditional appointments.
Past studies have shown that outpatient asynchronous consultations can provide care quality like in-person appointments but with more convenience and often at a lower cost. Even though the pandemic has ended, these consultations are likely to remain a service option. For them to be widely and fairly used, it is essential to understand how to effectively develop and use them in practice.
How did we study this?
Between April 2021 and July 2022, we engaged with NHS Grampian staff, patients, and the public. We sought to understand how people in Grampian felt about this new method of specialist consultation, paying particular attention to the opinions of older individuals, those with low incomes, and people with disabilities. We also spoke with staff who developed and used this service, and patients who were offered this service, about their experiences.
From January to September 2022, we surveyed all users of this new service. However, primarily those under the care of the pain clinic responded, sharing their satisfaction levels and experiences. We also examined who and how many people were utilising this new service.
What did we find?
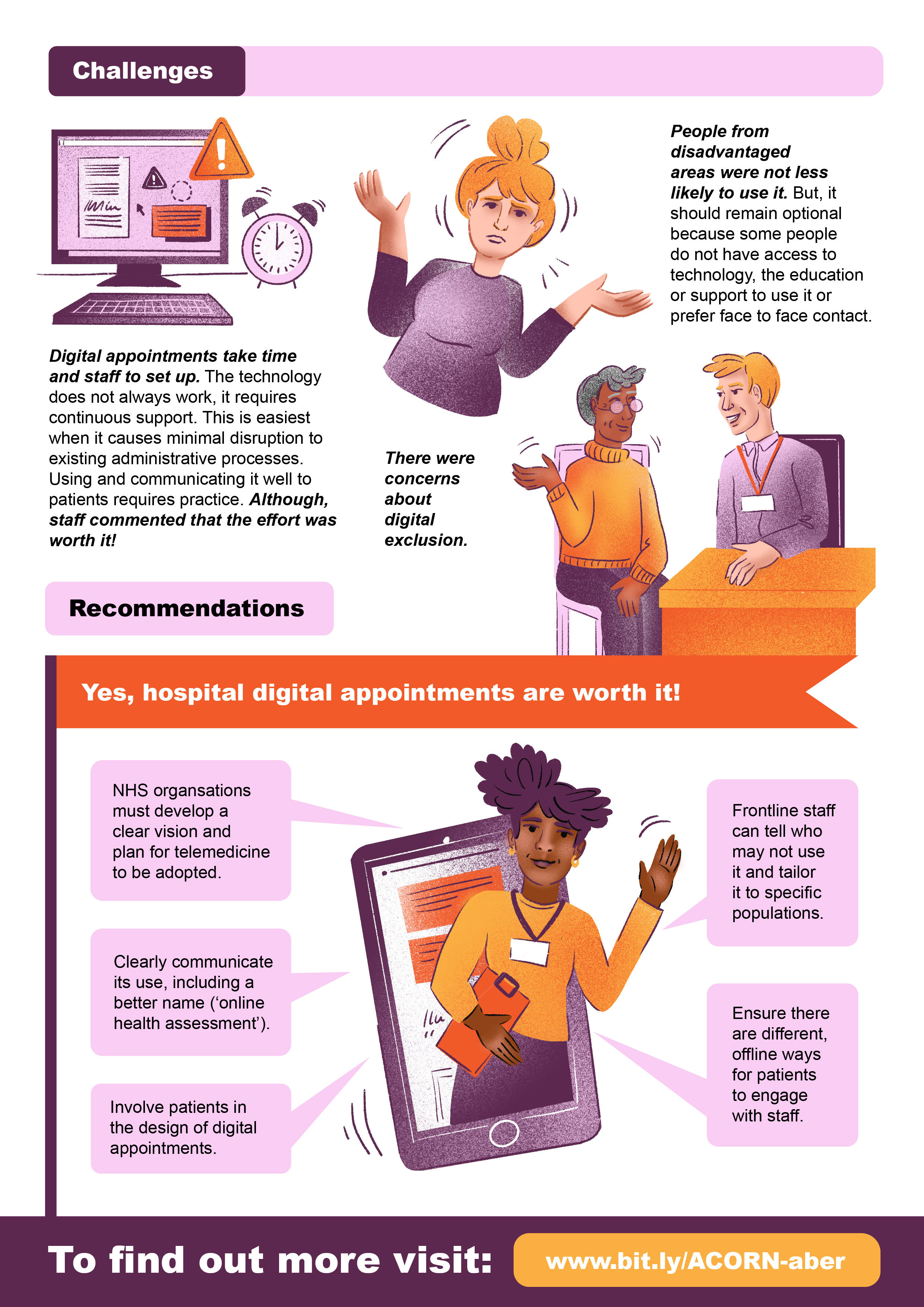
People from less wealthy areas attended ‘digital appointments’ and got treatments just as much as those living in more wealthy areas, which is reassuring. Over 1,417 people had nearly 1,709 appointments using asynchronous consultation for skin problems, stomach and intestine care, and pain management. Most users liked this new service, with 80% feeling neutral, happy, or very happy about it. Patients who used it told us that its ease of use helps to share information and offers doctors and nurses flexible schedules. Doctors and nurses agreed and highlighted that the service helps ensure the right patient connects with the appropriate clinical expert at the right time. The public believed it served as a valuable complementary service in Grampian, given its vast geographical area. Overall, the public felt positive about the potential role of this service, staff thought it was needed, and service users had mostly good experiences with it.
The study participants thoughtfully considered who this service might or might not be suitable for. The primary concerns of the public, staff and patients were the possibility of excluding some individuals and the loss of personal interaction. Clinics attempted to address these issues by carefully choosing their patient groups. Concerns were also raised about technical difficulties, a lack of devices, and digital literacy, which some service users indeed reported. We noted that some patients simply prefer face-to-face consultations, as they thought they could better express their needs in person. Overall, while efforts can be made to make the service more inclusive, it might not be suitable for everyone, especially those who are not tech-savvy or struggle with written communication. Therefore, it is important to continue offering patients a choice while working to reduce barriers to access. The service could be enhanced by providing a simpler explanation of its functioning and renaming 'digital appointment' to 'assessment' for clearer understanding.
When it came to staff opinions about integrating this service into everyday practice, there was hope at the beginning that rolling out a similar service between departments of the same hospital would be straightforward. Even with good support, the process of adopting this approach in new departments serving different populations of patients was challenging. This shows that expanding the approach and starting new services each come with their own set of challenges. However, over time, staff improved their ability to use the new service and explain it to patients. Even though numbers showed this service was effective across all departments, the pain management team found it easier to use, primarily because it resonated with their existing administrative process. To make it workable long-term, the service needs to be adaptable enough for various clinics, and there needs to be sufficient funding for its operation and to pay all the people who run the service, including clinical, technical, operational staff and clinical coordinator.
Outputs
Public contributors testimony: What it's like to be involved in implementation research: a personal testimony by Mike Melvin
The results of the ACORN study: Transforming outpatient care - assessment of Grampian's digital appointments

Contacts
- Magdalena Rzewuska; magdalena.rzewuska@abdn.ac.uk
Status
CompletedPublications
Rzewuska Díaz M, Locock L, Keen A, Melvin M, Myhill A, Ramsay C 'Implementation of a Web-Based Outpatient Asynchronous Consultation Service: Mixed Methods Study', J Med Internet Res 2024;26:e48092, URL: https://www.jmir.org/2024/1/e48092, DOI: 10.2196/48092