![]()
![]()
![]()
![]()
![]()
![]()
|
|
|
|
ProcedureThose who measure blood pressure should be familiar with the practical points listed and discussed below. Practical points
Explanation to patientThe observer should outline the procedure briefly. In particular, he or she should warn the patient of the minor discomfort caused by inflation and deflation of the cuff and tell the patient that the measurement may be repeated several times. White coat hypertensionIn many patients blood pressure is always higher when measured by doctors (and nurses) - this is the phenomenon of "white coat hypertension". Readings are likely to be lower when they are taken in the home or by ambulatory blood pressure measurement (ABPM).
24 h ABPM confirms the presence of white coat hypertension in this patient Defence reactionThe defence reaction is the rise in blood pressure associated with the anxiety of measurement. This increase in blood pressure tends to subside once the patient becomes accustomed to the procedure and to the observer. Changes in drug treatment should not be made on the basis of one measurement of blood pressure but rather on the patterns of blood pressure change during a period of observation. In many patients blood pressure levels fall without treatment. Variability in blood pressureBlood pressure varies in individuals according to the time of day, meals, smoking, anxiety, temperature, and the season of the year. It is usually at its lowest during sleep. Posture of patientWhether the patient is sitting or lying (supine) makes no difference to the blood pressure readings, provided that the arm is in the correct position. However, pressure should also be measured in the standing position in patients whose symptoms or drug regimen may be associated with a disproportionate postural fall. Pregnant patients may suffer a profound fall in blood pressure when lying supine; therefore in pregnancy all measurements should be performed with the patient either sitting or in the left lateral position. No information is available on the optimal time to be spent in a particular position before the measurement. We suggest 3 min lying or sitting and 1 min standing. Application of cuffThe patient should be in a warm environment. Tight or restrictive clothing should be removed from the arm. A simple measure is to request that patients wear a loose fitting, short sleeved garment when attending for blood pressure measurement. The position of maximal pulsation of the brachial artery in the arm, just above the antecubital fossa, may be marked lightly with a pen. A cuff with a long enough bladder should then be applied to the upper arm. As contact of the stethoscope with the tubing of the cuff may produce artefactual sounds, the tubing from the blood pressure cuff should not cross the auscultatory area. The centre of the bladder should be positioned over the line of the artery. The lower edge of the bladder should be 2-3 cm above the marked point. The cuff should fit firmly and comfortably and be well secured.
Position of armThe arm should be horizontal and supported at the level of the mid-sternum because dependency of the arm below heart level leads to an overestimation of systolic and diastolic pressures of about 10 mm Hg. Correspondingly, raising the arm above heart level leads to underestimation of these pressures.
Position of manometerThe mercury column of the sphygmomanometer must be vertical, at eye level, and not more than 3 feet from the observer. Stand mounted manometers are recommended, largely because they are mobile and easily adjusted for height. Box and desk models are more easily damaged and less convenient to use.
Estimation of systolic pressureThe systolic pressure should be estimated before the operator uses the stethoscope by palpating the brachial artery pulse and inflating the cuff until the pulsation disappears. The point of disappearance represents the systolic pressure. This measure is especially useful in patients in whom auscultatory end points may be difficult to judge accurately - for example, pregnant women, patients in shock, or those taking exercise. Auscultatory measurement of systolic and diastolic pressuresThe stethoscope is placed gently over the artery at the point of maximal pulsation. It must not be pressed too firmly or touch the cuff, or the diastolic pressure may be underestimated. The pressure is then raised by inflating the bladder to 30 mm Hg above the systolic blood pressure as estimated by palpation. Next the pressure is reduced at 2-3 mm Hg per second. The point at which repetitive, clear tapping sounds first appear for at least two consecutive beats gives the systolic blood pressure. The point where the repetitive sounds finally disappear gives the diastolic blood pressure (phase 5). Both measurements should be taken to the nearest 2 mm Hg to avoid digit preference. Auscultatory sounds
Summary of blood pressure measurementPalpatory estimation of systolic pressure
Auscultatory measurement of systolic and diastolic pressure
Digit preference, whereby observers choose to record a favourite number, most commonly 0 or 5 mm Hg, is a serious source of bias. It is important to realise that such digit preference may introduce substantial errors that could lead to incorrect decisions being made, especially in patients with borderline blood pressures. Such bias is best avoided by recording systolic and diastolic pressures to the nearest 2 mm Hg. The silent or auscultatory gap occurs when the sounds disappear between the systolic and diastolic pressures. The importance of the gap is that unless the systolic pressure is palpated first it may be underestimated. The presence of a silent gap should be recorded on the case sheet or blood pressure chart. Number of measurementsIt is preferable to take one measurement carefully at each visit, repeating the measurement if there is uncertainty or distraction, rather than to make several hurried measurements. If the blood pressure is elevated above say 140/90 mm Hg, a second reading should be recorded after an interval of at least 1 min. For patients in whom sustained increases of blood pressure are being assessed a number of measurements should be made on different occasions before definite diagnostic or management decisions are made. Sustained blood pressure elevation
Indications for measurement in both armsThe pulse should always be palpated in both arms. A difference between arm pulses may be a clue to coarctation of the aorta, anatomical variants and alterations to the pulse after surgical or cardiological procedures, such as cardiac catheterisation. Blood pressure should be measured in both arms in all patients with raised blood pressure at the initial assessment. It is suggested that if there is a reproducible difference of 20 mm Hg for systolic pressure and 10 mm Hg for diastolic pressure, decision making should be based on the limb with the higher pressure. Simultaneous measurement in both arms is indicated in patients with suspected coarctation of the aorta where local anatomical abnormalities are suspected. What to note when measuring blood pressure
Coarctation of aorta or suspected anatomical abnormalities
Times of measurement for patients taking drugs that lower blood pressureIn patients taking drugs that lower blood pressure the measurements may vary depending on the time of day at which the drugs are taken. It may therefore be helpful, when assessing the effect of antihypertensive drugs, to note the time of drug ingestion in relation to the time of measurement. Leaflet advicePatients with high blood pressure should be given a leaflet emphasizing that blood pressure elevation is only one risk factor for cardiovascular disease. Giving up cigarettes, reducing alcohol consumption, weight reduction and dietary restriction of cholesterol and fats may be as important as lowering blood pressure.
[Home] [Introduction]
[Procedure] [Obtaining
a blood pressure profile] [Equipment] © BHS 1999 |

 Video
Video
 Video
Video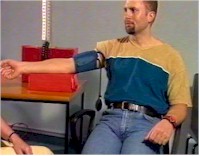 Video
Video
 Video
Video Video
Video Video
Video Video
Video